BiteSized Immunology: Pathogens & Disease

Human Cytomegalovirus (HCMV)
HCMV-associated disease
Human cytomegalovirus (HCMV) is a beta-herpesvirus that causes lifelong infection in humans. HCMV has a prevalence of 55-100% within the human population, depending on different socioeconomic and geographical factors. Primary HCMV infection is generally asymptomatic in healthy hosts but can cause severe and sometimes fatal disease in immunocompromised individuals and neonates. HCMV is the leading infectious cause of congenital abnormalities in the Wwestern world, affecting 1-2.5% of
all live births. HCMV intrauterine infection and can cause significant morbidity, including low birth weight, hearing loss, visual impairment, microcephaly, hepatosplenomegaly, and varying degrees of mental retardation.
HCMV also causes serious disease in organ transplant recipients and AIDS patients, either after primary infection or reactivation of latent infection. In immunocompromised individuals, HCMV infection is often controlled by early treatment with antivirals but problems exist such as toxicity, the emergence of antiviral-resistant HCMV strains and the availability of antiviral drugs in developing countries.
The immune response to cytomegalovirus
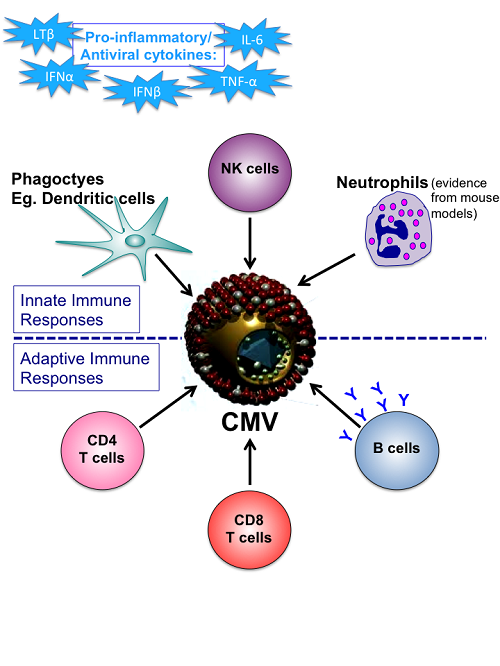
Extracellular and intracellular pathogen recognition receptors, such as Toll-like Receptors (TLRs), recognise components of the virion, which triggers the innate immune response to the virus. This leads to the production of inflammatory cytokines, such as type 1 interferons (IFN), tumour necrosis factor alpha (TNF-α) and interleukin-6 (IL-6). These inflammatory cytokines can recruit and activate phagocytic cells, such as dendritic cells, which can engulf HCMV-infected cells. Natural killer (NK) cells are also recruited to initial sites of infection and eliminate HCMV-infected cells by the release of cytotoxic proteins, which destroy target cells. Furthermore, data from the murine cytomegalovirus (MCMV) model of infection suggests that neutrophils contribute to early control of virus infection.
The adaptive immune response contributes to the long-term control of HCMV. HCMV infection results in an extremely large cytotoxic CD8 T cell response that appears to be crucial for the control of primary HCMV infection and reactivation from latency. Also, HCMV-specific IFN-γ-secreting CD4 T cells are associated with decreased virus shedding into urine, thus limiting its spread to new hosts. B cells also play a role in controlling HCMV infection and may also help prevent its transmission to new hosts as maternal antibodies can confer protection to foetuses in utero.
A summary of the immune responses to HCMV is shown in Figure 1.
Immune evasion by HCMV
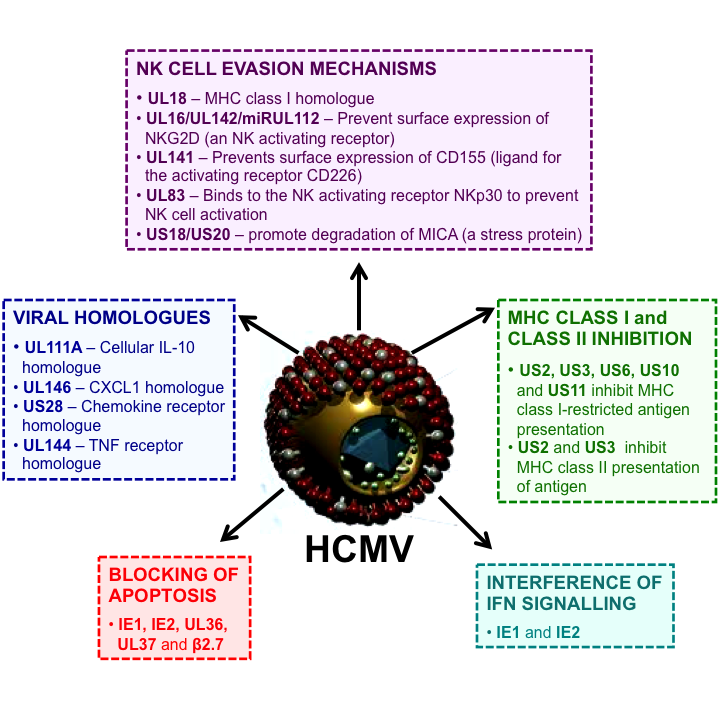
HCMV has co-evolved with humans for millions of years. During this time, it has acquired a number of different mechanisms that modulate and evade the human immune response, which allows for more efficient infection and dissemination within the body. HCMV dedicates a large proportion of its genome to down-regulating NK cell activity. The HCMV UL16 and UL142 proteins prevent the expression of NK cell activating ligands on the surface of infected cells, while the HCMV UL83 can bind directly to NKp30, an activating NK cell receptor, and prevent activation of the NK cells. Furthermore, the HCMV US18 and US20 proteins promote the degradation of MICA (a major stress protein), preventing the NK cell from recognising stress signals of an infected cell. HCMV has acquired a viral homologue of IL-10, an immune modulatory cytokine that has been demonstrated to suppress anti-cytomegalovirus immunity. HCMV also targets the activation of the adaptive immune response. The HCMV US11, US2 and US3 proteins down-regulate the expression of major histocompatibility complex (MHC) class I and II molecules on cells, such as antigen presenting cells, which prevents the presentation of HCMV-derived peptides bound to MHC molecules to unstimulated T cells, a process required for the activation of T cells.
Virus infection of cells can trigger apoptosis of the human cell, a programmed cell death mechanism that is important for limiting the spread of the virus. These apoptotic cells are then cleared by phagocytic cells, thus preventing the release of new virions. However, HCMV has evolved proteins (UL36 and UL37), which prevent apoptosis of infected cells, promoting its dissemination within the host. A summary of immune evasion mechanism employed by HCMV is outlined in Figure 2.
Despite the plethora of immune evasion mechanisms developed by HCMV, the human immune system still produces a robust immune response in response to this virus. This is clearly demonstrated by the fact that most primary infections in immunocompetent hosts are asymptomatic and that HCMV disease occurs mainly in those with compromised or immature immune systems. Current research aims to fully elucidateing the mechanisms by which HCMV manipulates the human immune system in order to improve antiviral therapies and to develop a vaccine capable of boosting the initial antiviral immune response, thus preventing the establishment of HCMV infection.
© The copyright for this work resides with the author