BiteSized Immunology: Pathogens & Disease

Chronic Obstructive Pulmonary Disease
Chronic Obstructive Pulmonary Disease (COPD) is a diverse respiratory disorder whose main characteristics include the persistent obstruction of the small airways of the lungs, the destruction of alveolar tissue and chronic bronchitis. It is estimated that about 328 million people suffer from COPD worldwide, but this number will soon rise significantly. The disease is projected to rank third in the most fatal disease table by 2020 and predicted to account for 7% of total deaths by 2030. COPD affects men and women equally, and with an onset at the age of 30-40 years it progressively diminishes life quality. This feature has also important consequences on state economics given that patient hospitalisation and treatment costs are considerably high.
The origins of COPD are mainly environmental, although genetic factors have also been shown to play an important role with deficiency of the protease inhibitor α1-antitrypsin being identified as a major genetic link to COPD progression in humans. Cigarette smoking has been primarily associated with the condition, while exposure to occupational toxic gases or dust, the use of biomass fuel, outdoor pollution and the socioeconomic status of the affected subjects can also cause COPD. The importance of environmental factors for COPD development is reflected on the spread of the disease; it is more prevalent in the industrialised countries of Europe and North America and developing countries of South American and Western Pacific regions. However, these figures are only speculative as the lack in diagnosis consensus and the frequent misclassification of other respiratory diseases makes it challenging to accurately estimate COPD prevalence.
Patients with COPD experience various symptoms the severity of which depends on disease stage. Chronic, progressive dyspnea (shortness of breath for more than one month) is the most characteristic one, with cough and sputum production being reported in one third of patients. COPD is particularly known for its heterogeneity and thus airway limitation very often does not coincide with shortness of breath and sputum production. In addition, some patients may demonstrate chest tightness and wheezing which adds another layer of complexity to proper diagnosis. Finally, patients with severe COPD sometimes suffer from fatigue, weight loss and anorexia which correlate with disease exacerbations due to bacterial and viral infections. It is therefore important that clinicians consider multiple factors to correctly diagnose COPD.
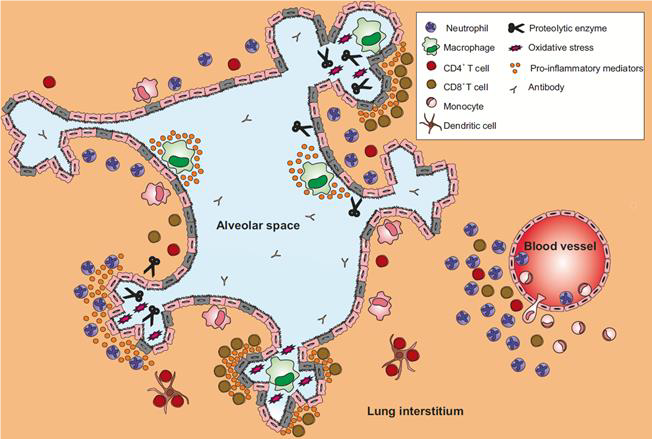
COPD is triggered when injured bronchial epithelial cells release pro-inflammatory mediators in order to recruit leukocytes to the site. Blood neutrophils, monocytes and lung-resident alveolar macrophages are the first responders and together they create a highly inflammatory micro-environment via the secretion of cytokines, chemokines, reactive oxygen species and proteolytic enzymes. Dendritic cells have also been found in the lungs of patients, whilst the role of eosinophils has not yet been elucidated. The priming of innate immunity leads to the activation of adaptive immune cells. It is not yet clear what causes their mobilisation to the lungs of patients with COPD; oxidative stress as well as autoimmune mechanisms have so far been put forward as potential molecular mechanisms, but more investigation is needed to tackle this research question. CD4+ T helper cells differentiate into the TH1 and TH17 phenotypes, while cytotoxic CD8+ T cells, which are predominant in the lungs of patients, induce epithelial cell death. Finally, some studies have detected autoantibodies in the bronchoalveolar fluid of patients with COPD, which implies the presence of B cells in the tissue.
Despite the combined efforts of the academia and the pharmaceutical industry, there are no available treatments that fully reverse the airway obstruction observed in COPD. Current therapeutics aim to relieve the symptoms and reduce the frequency and severity of disease exacerbations. Bronchodilators are the first-choice maintenance option for mild COPD, whereas combination therapies with corticosteroids are used to attenuate lung inflammation in patients with severe COPD and exacerbations. However, the emerging epidemiology of the disorder makes it mandatory that we design effective therapies for patients with COPD. In fact, several targets are currently considered, some of which are in early clinical trials, such as phosphodiesterase inhibitors, interleukin receptor and signalling kinase inhibitors.
© The copyright for this work resides with the BSI.