BiteSized Immunology: Pathogens & Disease

Respiratory Syncytial Virus (RSV)
Importance
Respiratory Syncytial Virus (RSV) is a major cause of disease in childhood and old age, with symptoms ranging from a common cold to bronchiolitis and pneumonia. An estimated 160,000 – 200,000 deaths globally can be attributed to RSV infection. The burden on healthcare infrastructures is significant, and in the U.S. it is estimated to cost $600 million per year. Even though most children are exposed to RSV within the first two years of life, lifelong re-infection with RSV is common, even within the same season and sometimes with the same strain. Full and long-lasting immunity does not develop despite repeated exposure, and although almost everyone has anti-RSV antibodies, these are often poorly neutralising. Risk factors for severe RSV disease include premature birth, old age, congenital lung or heart disease, T cell immunodeficiency, birth order (in relation to other siblings) and birth season. However these factors do not guarantee severe disease and absence of these factors does not guarantee mild disease, suggesting there are underlying genetic susceptibilities.
There is no specific treatment for RSV, although the monoclonal antibody Palivizumab, which targets the F protein, can be used to prevent infection. However, this treatment is very expensive and it is only administered to very high risk babies. For most other hospitalised cases, supportive care is given consisting of breathing support and fluid replacement.
The Virus
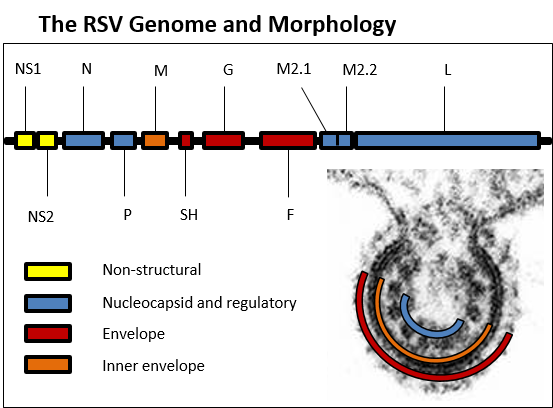
RSV is a negative-sense single-stranded RNA paramyxovirus consisting of 10 genes producing 11 proteins. There are two antigenic subgroups (A and B) that differ in the hypervariable region of the G protein gene. RSV largely infects lung epithelial cells through attachment of the F and G glycoproteins. The external F and G allow the virus to attach to its target cell via TLR4 and/or nucleolin. Infected cells can merge via the displayed F proteins on the cell membrane, forming characteristic syncytia. The surface proteins (F and G) are believed to be the best targets for a vaccine, especially for the induction of antibody.
The RSV Genome and Morphology
Who needs a vaccine?
Vaccines need to be targeted at distinct at-risk groups. Infants between 0-6 months are at the greatest risk of severe RSV disease symptoms and therefore in need of greatest protection. However, an immature immune system makes vaccinating this age group challenging.
Children over 6 months old are better able to respond to vaccination and still comprise a significant group of disease burden, especially in the developing world. Also, since they represent a reservoir of infection for new-borns, a vaccine targeted to this group may be reduce the burden of RSV.
Pregnant women could also be targeted in order to induce immunity so that antibodies are passively transferred to the infant via the placenta and then via breast milk following birth. This would help to protect infants during the first few months of life.
The final vaccine target group are the elderly who have an aging immune system that needs to be boosted in order to protect them from serious complications of infection.
A Troubled Past. The FI-RSV Vaccine
In the 1960’s, a clinical trial evaluated the effects of a formalin-inactivated (FI), whole virus RSV vaccine that was administered to infants and young children. Formalin inactivation had been successfully used to produce a variety of safe and effective viral vaccines, for example, polio. However, the FI-RSV vaccine had disastrous consequences as not only was it poorly protective, but it also primed for vaccine-enhanced disease that resulted in the death of children upon natural exposure to the virus. Later studies revealed that enhanced disease occurred in part due to induction of poorly neutralising antibodies and a Th2 – biased CD4 T cell response. However, complete mechanisms of this are not fully understood. This legacy of vaccine enhanced disease has meant that vaccine safety is key and regulatory hurdles are significant.
Current Vaccine Development
Vaccine development for RSV has been ongoing for over 50 years. Many vaccination approaches have been tested and these can be divided into these four categories: 1) whole inactivated viruses 2) live attenuated viruses 3) gene based vectors and 4) subunit and particulate forms of RSV antigens. These approaches have been unsuccessful due to a combination of factors: correlates of full protection are unknown, the requirements for generating a long lasting memory response are not known, vaccine efficacy for human use cannot be fully predicted via animal models, protection needs to be instigated against both serotypes of RSV and it is of utmost importance to avoid the possibility of vaccine enhanced disease and immunopathology. However, promising candidates include a live-attenuated strain devoid of the gene encoding the small hydrophobic (SH) protein with additional genome mutations, and a modified pre-fusion form of the F protein displaying immunodominant epitopes. It is likely further candidates will reach human testing in the near future.