
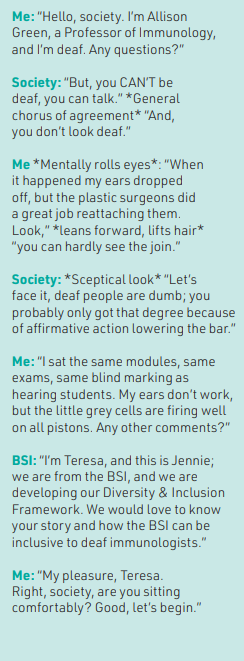
At the BSI we are committed to working hard to foster a culture within immunology that ensures fair treatment and opportunity for all. Here, Professor Allison Green, from University of York, shares her experience being deaf and having a career in immunology, and highlights the important obstacles for deaf people in society as well as tips for helping deaf researchers.
I had a typical childhood; boisterous, fun, active. I excelled at school. Easter recess 1979, the family holidayed in Majorca. Sun, swimming, laughter, magical. Towards the end of the week, I developed sudden onset of an excruciating headache, vomiting, my neck immovable. “Just sunstroke,” said the hotel doctor, “but I’ll give her some penicillin just in case”. I rapidly deteriorated, my mum – a nurse – insisted it was more than sunstroke. An ambulance was called, and I drifted into unconsciousness to the sound of its siren. Unbeknown to me, it was the last sound I would ever hear. I contracted meningococcal meningitis, and consequently, the hairs in my inner ears that are essential to transmit sound were destroyed. I was 11 years old. It was a long road to recovery; learning to lip-read, talk, walk again. But children are resilient, accepting. Adults, sadly, less so. My parents faced a cacophony of voices from educationalists: “Deaf people are intellectually impaired”, “Institutionalise her”, “She hasn’t a future”. They fought hard for my right to an education; a deaf child in mainstream schooling was unheard of. I owe them everything, and in autumn 1979 I joined my friends at secondary school. At school I thrived, helped by access to books and teachers who believed in me.
Higher education
Whilst the doomsayers still spilled their bile, “you need a reality check, deaf people don’t go to university”, their voices grew weaker, and as a wide-eyed 18-year-old I entered Glasgow University to study biochemistry. In my experience, the Science Faculty at Glasgow University was ahead of the times in inclusivity; whilst another university I applied to focused my interview on all the reasons a deaf person should not do science but stick to the “easy subject of humanities”, my interview at Glasgow focused solely on my needs, and how they could help me succeed. I had no hesitation in accepting their offer.
As a kid from a small country town, I adored Glasgow; both educationally and socially. I coped in lectures by asking the person next to me if I could copy their notes, I found lipreading a challenge due to poor lighting, and suddenly losing track as they turned to use the blackboard. For effective lipreading, the face should not be in shadow, and eye contact with the lipreader is vital. Nevertheless, with peers’ notes, books, and attentive lecturers in lab practicals, I managed. Transitioning from 2nd to 3rd year is preceded by a nominated lecturer, i.e. whoever pulled the short straw, to hang out their shingle and entice students to select their subject to graduate with honours. Talks on genetics, biochemistry, microbiology, etc. made my eyes close, as tiredness engulfed me trying to assimilate all the information. Then, the immunologist stood up; he talked about disease, and this incredible entity that surges through our bodies to protect us – I was mesmerised.
Falling for immunology
Entry was highly competitive, with 16 places for scientists, four for intercalating medics. I worked so hard in my 2nd year exams to attain the marks I needed, and, following an interview with David Stott, I was rewarded with a place. I was ecstatic. The 20 students and lecturers quickly became what I can only describe as a close-knit family unit.
Immunology is complex, and as a deaf person, I learn through imagery not by the spoken word. Like many deaf people, I sometimes struggle with reading (and writing); although I can read every word in a sentence, I don’t always understand the meaning of the sentence on the first readthrough. This is also true for conversations, and often when I ask someone to repeat something, it is due to confusion of the meaning of what they said, not the words spoken. So, understanding MHC-peptide selection became fitting different-sized eggs in an egg box; random rearrangements of the B-cell receptor and T-cell receptor became different ingredients in a cake, dependent on the type of cake you want to bake. And so on. This imagery learning is central to my teaching of immunology to students and public speaking; my colleagues have got used to student essays describing chemokines as ‘immunological sat navs’ – much to their dismay at times!
Like previous years, practicals were where my real passion for immunology shone. First in the queue to enter the lab, and last to leave. I adored the innovation and the intricacies of research. I was fortunate to attain a Wellcome Trust Vacation Scholarship to spend a summer in Allan Mowat’s lab researching Graft-versus-host disease (GvHD), and for my final year project I selected Bill Cushley’s lab to study B-cell responses to cytokines. I had no doubt my career path would be research.
Next steps
As our degree ended, my peers excitedly showed letters from institutes offering them interviews for PhD studentships. “What about you, Allison?” they asked. “Oh, I am still thinking what I will do next,” I would say. I didn’t want to dampen their joy by telling them the same institutes that were offering them interviews were sending me letters saying the positions were filled. I always felt transparency was important, and I explained in my applications that I was deaf, but I could talk and my deafness wouldn’t impede my ability to do a PhD. But my protestations fell on ‘deaf ears’. Just when I was starting to lose faith, I was invited to interview for an MRC studentship at St Andrews University supervised by Rick Randall.
Rick, a virologist, had a project to develop a vaccine to Simian Immunodeficiency Virus (SIV), in the hope it would offer insights into vaccination against HIV. I was intrigued, and instinctively, I felt Rick would be a good supervisor. He offered, and I accepted the studentship without reservation. Rick was indeed an exceptional supervisor and I hope that I implement his ethos in my own supervision of graduate students. Active research presented some challenges – impervious to sounds indicative of e.g. imbalanced centrifuges, or failed fume hood extractors, I learned through the sense of touch-unique vibrations, if equipment was working properly.
A difficult decision
Life trundled on, when out of the blue I received a letter from my former ENT consultant. There was a ‘new’ operation called a cochlear implant. It was for deaf people whose inner ear (cochlear) was damaged and couldn’t use conventional hearing aids that simply magnify sound. Would I consider it? You may think my answer was a rapid “Yes”, but it was one of the most difficult of decisions I have had to make. Ardent and vocal in my condemnation of doomsayers’ discrimination of deaf people’s worth to society/academia, I thought that surely to accept made me a hypocrite. The deaf society vehemently condemned cochlear implants as cultural genocide. It was a difficult time in my life, but after a lot of sole searching, I said “Yes.” So, in my final year of my PhD, 26 years old, I became the 200th patient of a cochlear implant in the UK.
That year is a blur; the operation and aftercare were in Manchester Royal Infirmary; weekly appointments for many months as they trained my brain how to understand speech and everyday sounds, whilst furiously trying to complete my PhD. Rick and my colleagues were amazingly supportive. I was fortunate, I adapted well to the implant, and it really aided lip-reading; in essence I ‘hear’ half the word and lip-read the rest. I progressed from understanding 60% of speech through lip-reading, to 98% by combined lip-reading and the implant.
From despair to delight
During this time, like my cohort, I was sending out letters for postdoctoral positions. Still being transparent, I would mention my deafness, but that I could talk. I received no replies. I was, and will always be, deaf. A cochlear implant is simply a sophisticated hearing aid; it does not magically take your deafness away. One day Rick called me to his office. He asked how the job hunting was going. “Slowly,” I replied. He sighed. He told me he had been phoning all his contacts, including people I had written to, and all were universal in saying, sorry, but they wouldn’t employ a deaf person. It would be too disruptive for the lab. I couldn’t move, couldn’t breathe. “But, I can talk” I said. “I know, I explained that” he replied. “But, I’ve completed a PhD” I said. “I know, I’ve tried. Really tried to make them see sense. And I am sorry, but I think you need to prepare yourself for the fact that you won’t get a job.” He looked devastated. I felt so defeated. All my aspirations gone. No matter how talented a researcher, number of papers published, the realisation that all these PIs saw was the deafness and perceived impediment – something I could not change – overwhelmed me. I went home and cried.
Willie Russell was our Head of Department, and one day gave me the Howard Hughes (a USA equivalent of the Wellcome Trust) tome detailing all their funded immunologists – the immunologist’s ‘who’s who’. I happened to mention Richard Flavell’s research looked interesting. “Leave it to me,” and off he went. Life trundled on, thesis writing. One day a letter arrived, it was from the CDC in Atlanta offering a position to study influenza virus – one of Rick’s contacts had at last come through. This was immediately followed by a letter from Richard Flavell offering me a postdoctoral position at Yale School of Medicine. I could not believe how lucky I was.
Challenges of networking
I accepted Richard’s offer, focusing on research into the immunopathology of type 1 diabetes. I am fortunate that my postdoctoral training was productive with a series of fellowships, high profile papers and conference presentations. At the heart of my successes, was Richard – blind to my deafness, he only saw potential and he created an environment where I could shine. He talked about my research far and wide, always crediting me throughout the talk. I have learned to do that for my own postdoctoral research associates. I regard Richard as an incredible mentor, and a friend.
By the end of my postdoctoral training, there were no issues finding jobs; people only cared about my aptitude for research. I moved to Cambridge University, setting up my own laboratory funded by the Juvenile Diabetes Research Foundation (JDRF) and Wellcome Trust, and subsequently moved to Hull York Medical School, University of York on a Wellcome Senior Research Fellowship. Here, I have tenure. My deafness had no impact on the everyday running of the lab, teaching, training the next generation of researchers, or interacting with colleagues. Networking on the international scale, though, was challenging. The inability to use conference calling, and the inaccessibility of noisy scientific meetings negating the use of my implant, restricted building collaborative networks, which is so essential for boosting one’s CV. Of course, there was email, but it is difficult to maintain a successful collaboration through email alone. Sadly, this has resulted in some reviewers of grant proposals commenting on my lack of productivity and scoring me low, and I think grant panels need to understand that the playing field is not level for disabled researchers. Now, however, since the COVID-19 pandemic and the explosion of Zoom/Teams with live closed captions, the national and international world is opening to me, and I have some wonderful collaborations ongoing now. But there is much more to be done.
Challenges ahead
I do not see myself as inspirational; my ears don’t work; the little grey cells still fire on all pistons. Deaf does not equate to being dumb. It is simply a communication issue. As many deaf students have the grades to attend Russell Group universities as hearing students, yet only 9% are offered positions, compared with 17% of hearing students. And of deaf students attending university, many document the lack of resources; notetakers, loop systems to help them integrate. The dropout rate is high. It has been 37 years since I started university, how can it be, deaf students are still struggling to get a higher education? How many incredible scientific minds and future discoveries have we lost, by lack of investment in the deaf person’s needs? And let’s face it, their needs are rather simple. If organisations wish to push their equity, diversity, and inclusion (EDI) policies, they should remember that EDI does not just refer to gender identity or ethnicity.
It isn’t easy to live the life of a deaf person. You face discrimination on many levels by misguided members of society. However, I feel privileged to be deaf; it has enabled me to meet so many incredible people – colleagues, tutors, mentors, students – whose collective, supportive voices soar. Whatever achievements I have made, and will make, is credit to their belief in me. And that, Society, is my story.
Professor Allison Green, Hull York Medical School, University of York
Top tips to help deaf researchers
Lip-reading
- Make sure you stand with the light facing you.
- Make eye contact, the whole face is lip-read, not just the lips.
- Speak normally, don’t shout, but keep sentences short.
- If the person is struggling to understand you, think of rephrasing the sentence with different words.
- Don’t be offended if a deaf person speaks abruptly or ‘to the point’. This is how language is perceived by the deaf.
- Natural ending of sentences is not apparent when lip-reading. Don’t be offended if the deaf person seems to keep butting in.
- Do let them know the subject, and don’t quickly change it. Lip-reading relies on the brain knowing the subject to make sense of the words.
Conferences
- Ask the deaf person what their needs are; we all have different needs, e.g. some might need sign language interpreters.
- Make sure the speaker’s face is well lit.
- Speakers should face the audience, not the screen.
- Use the microphone, it interacts with the loop system, but note, not all hearing aids are compatible with loop systems.
- Ask the deaf person beforehand where it is best for them to sit – there is a sweet spot for loop systems to work. Don’t assume the front row is best, usually it means the computer hides the speaker’s face.
- Do think about incorporating software where audience questions are shown on a screen and, Chairs, remind speakers to repeat questions.
- Designate a ‘quiet’ area where the posters are for the deaf person to communicate; normally the noise in these poster presentations is distracting.
Funding agencies
- Don’t ask someone to tick a box if they have a disability, then give them no scope to explain what impact it has had on their career. We are more than ‘ticks in boxes’ to fulfil your EDI policy.
- Do appreciate that CVs from disabled researchers may be lighter than abled-bodied researchers due to living with their disability, e.g. hospital visits, challenges of networking where oral communication/ conference calling is utilised. Zoom/ Teams with closed captions have only been available post-COVID. It is not a reflection on their intellectual capabilities.
- Do understand that disabled researchers are not looking for ‘an easy ride’. Research proposals should always be reviewed as rigorously as an abled-bodied researchers.