BiteSized Immunology: Immune Dysfunction

Inflammatory Bowel Disease
Inflammatory bowel disease (IBD), comprising Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic, relapsing-remitting inflammatory disorder of the gastrointestinal (GI) tract. CD and UC vary in the region of the GI tract they affect; the extent of inflammation and resulting tissue damage; and their associated symptoms. UC tends to exhibit continuous superficial inflammation which spreads from the rectum and is limited to the colon (large intestine), with bloody diarrhoea as the most common symptom. Inflammation associated with CD is transmural (affects all layers of GI tract tissue), patchy (areas of inflammation are interspersed with healthy unaffected tissue) and can present anywhere along the entire GI tract and, in some cases, in the skin and joints. The symptoms of CD are more diverse than for UC, including diarrhoea, abdominal pain and weight loss.
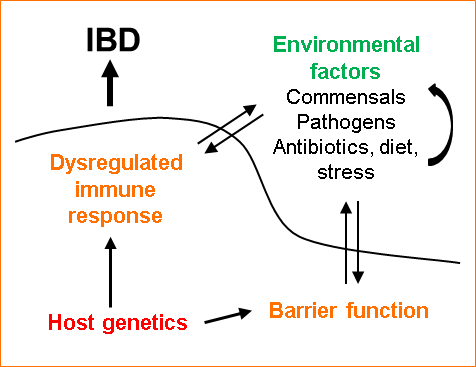
The exact cause of IBD is unclear. There appear to be four main factors which influence the disease: host genetic susceptibility, a dysregulated immune response and impairment of intestinal epithelial barrier function, and environmental factors (Figure 1).
Genetic susceptibility
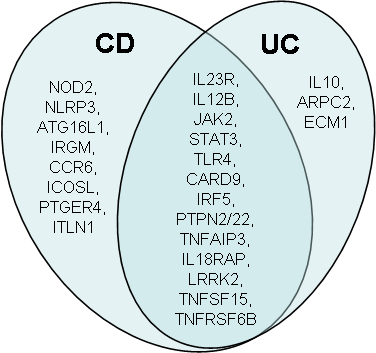
Genome-wide association studies (GWASs) have identified a number of genetic loci associated with IBD, including genes specific to either CD or UC, and some which are common to both (Figure 2). The risk of developing IBD conferred by variants at each locus is small for all but a few genes (e.g. IL10RA and IL10RB). It may be the case that IBD only occurs when multiple genetic variations associated with the disease are present. Another possibility is that environmental factors are required to trigger the onset of disease in genetically susceptible individuals.
Environmental factors
Environmental factors such as the commensal microflora, pathogenic infections and metabolic factors are thought to play a role in the development and perpetuation of IBD. The intestinal microbiota, which is dominated by bacteria, but also includes viruses, fungi and protozoa, is crucial for development of the host immune system but also appears to be the target of the inflammatory response during IBD. The composition of the intestinal microbiota appears to be altered during disease, although whether this causes, or results from, intestinal inflammation is unclear. The effects of antibiotics, pathogenic infections and diet on IBD might be explained by their impact on the commensal microflora.
Dysregulated immune response
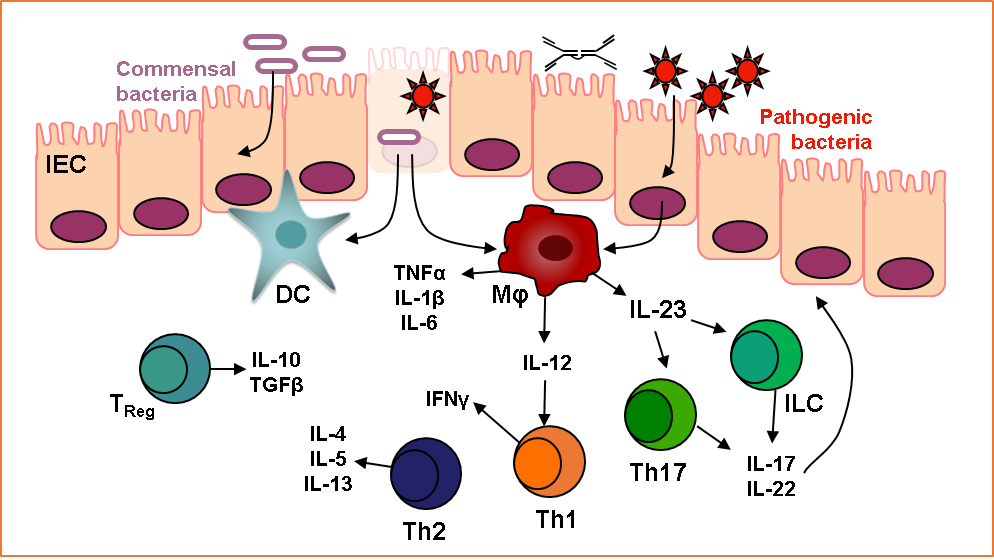
IBD is an immune-mediated disease, but is not considered to involve autoimmunity. The intestine contains an enormous antigenic load derived from the food and microbial flora present. Of the approximately 1014 bacteria in the intestines, the majority are harmless commensals which are beneficial to our health in numerous ways such as aiding digestion and preventing the colonisation of pathogenic species. The intestinal immune system is separated from this luminal content by a single epithelial cell layer, and must initiate the appropriate response – tolerance or protective immunity – upon exposure to each antigen. IBD is thought to arise when an inappropriate immune response is mounted against commensal bacteria. GWASs and experimental results have indicated a number of facets to this dysregulation, for example pro-inflammatory pathways driven by IL-23, decreased immune regulatory mechanisms, and defective barrier function of the intestinal epithelium. Figure 3 shows some key cell populations and mediators thought to be involved in intestinal inflammation. Monoclonal antibody-mediated blockade of the pro-inflammatory cytokine TNFα is very effective at reducing disease in many cases of IBD, highlighting a key role for this molecule in intestinal inflammation. Patients with disease refractory to this treatment, which is only employed after the failure of other therapies such as non-steroidal anti-inflammatory drugs (NSAIDs), corticosteroids and immunosuppressants, necessitate the discovery and development of novel therapeutic strategies.
Key references
Maloy and Powrie. 2011. Intestinal homeostasis and its breakdown in inflammatory bowel disease. Nature.
Kaser, Zeissig and Blumberg. 2010. Inflammatory Bowel Disease. Annu. Rev. Immunol.
© The copyright for this work resides with the author.