BiteSized Immunology: Pathogens & Disease

Chlamydia Trachomatis
The authors are funded by Tommy’s the Baby Charity
Chlamydia trachomatis (Ct) infection is the commonest bacterial sexually transmitted infection worldwide (Howie et al., 2011a, 2011b). In the under-25 age group in the UK 7–8% of men and women are infected (http://www.chlamydiascreening.nhs.uk/ps/index.asp). 70% of women and 50% of men who have Ct infection have no symptoms (Manavi, 2006); therefore if they do not get tested and treated, they can continue spreading the disease to their partners. These aspects of Ct infection can account for the distress that may occur when someone who had assumed that they were healthy, as they had no symptoms, discovers that they are infected when they happen to be tested for sexually transmitted diseases (STDs).
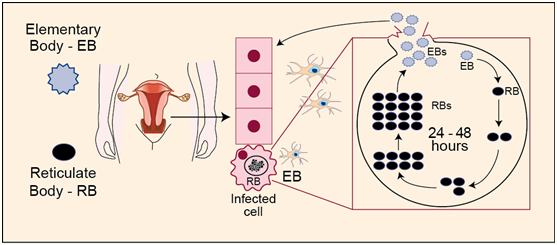
Life cycle of Ct in the human body
Ct is a Gram-negative bacterium which exists in two forms: the infectious elementary body (EB) and the intracellular reticulate body (RB), which is able to replicate and multiply. Infection begins when EBs attach to the membrane of a cell of the inner layer (epithelium) of the urogenital tract (Figure 1). EBs enter the cell and two hours later are transformed into RBs which grow and divide over the next hours, resulting in a rapid increase in number. At this point RBs transform into EBs. Usually, 48–72 hours after infection, the host cell bursts to release the infectious EBs (Hafner et al., 2008).
More than just a simple infection
Ct has a number of serovars which cause different types of pathology; A–C are responsible for ocular infections (trachoma) and are a major cause of blindness particularly in the developing world; D–K cause the common sexually transmitted infection and L1 and L2 cause the severe pathology of lymphogranuloma venereum.
In men, untreated sexual transmitted Ct can cause complications such as urethritis (Stamm and Cole, 1986) and chronic prostatitis (Skerk, 2003). Studies have also shown that men with Ct have poorer quality sperm compared to healthy counterparts (Hosseinzadeh, 2003). However, in women infection can have devastating and long-term effects on reproductive health. Ct has been associated with urethritis, pelvic inflammatory disease, scarring in the pelvis (such as adhesions), and fertility complications including ectopic pregnancy, infertility, miscarriage and premature rupture of membranes (Paavonen and Lehtinen, 1996; Falk et al., 2005; Wilkowska-Trojniel et al., 2009; Baud et al., 2011; Shaw et al., 2011).
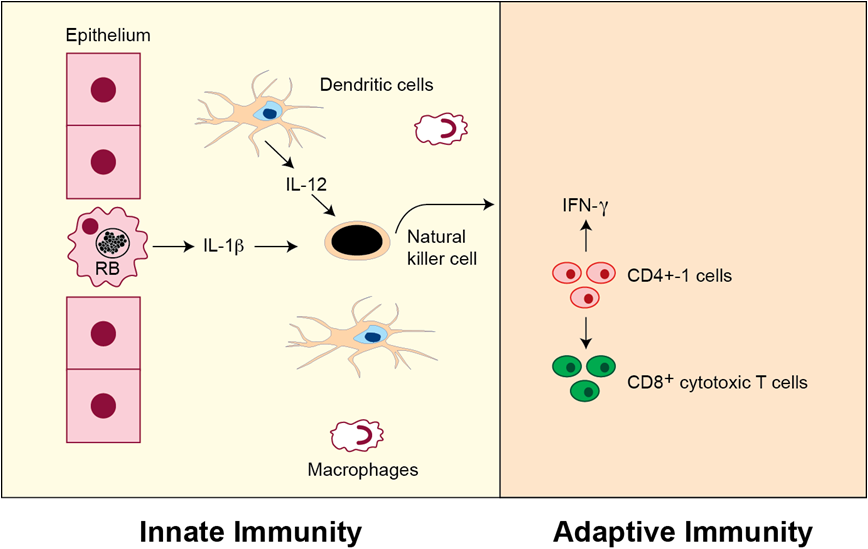
Mechanism of the immune response to Ct in women
Normally the female reproductive tract does not have associated organised lymphoid tissue but there are dendritic cells, macrophages and a few resident lymphocytes scattered throughout the four main epithelial areas, the vagina, the cervix, the uterus and the Fallopian tubes (Givan et al., 1997). Ct infection usually occurs in the lower genital tract and attracts different types of immune cells such as lymphocytes, macrophages and dendritic cells to infiltrate the epithelium. At the site of infection there is a strong inflammatory reaction mediated mainly by CD4+ T cells with a Th1 phenotype to clear the infection (Loomis & Starnbach, 2002, Figure 2). These cells produce interferon-γ (IFN-γ) which is known to inhibit chlamydial reproduction (Perry et al., 1997). However, there is evidence that the concentration of IFN- γ is critical to the outcome of infection; high levels of IFN- γ are associated with the clearance of the infection whilst low levels can allow the bacteria to persist without replicating. Ct infection can persist for several years and reinfection is common. It has been shown that reinfection can result in a strong secondary immune response and the increased inflammation may cause further damage to the reproductive tract. This has been suggested to be the case in chronic pelvic inflammatory disease (Hillis et al., 1997). If the infection spreads higher up the tract to the uterus and Fallopian tubes, the risk of ectopic pregnancy and infertility due to tubal damage is high. It remains unclear how much damage is caused by Ct and how much by the host immune response (Shaw et al., 2011).
Diagnosis, treatment and prevention
Ct is diagnosed by urinary testing or genital swab. It is treated with antibiotic therapy, such as azithromycin or doxycycline (http://www.nhs.uk/Conditions/Chlamydia/Pages/Treatment.aspx). There is concern that widespread use of antibiotics reduces the individual’s ability to make a proper protective immune response, although the correlates of protective immunity are themselves not well understood. There is currently no vaccine for Ct. Much more research is needed to understand the balance between the immune response and the growth of the organism to develop more effective ways of controlling this infection and preventing the reproductive dysfunction that it is associated with.
Bibliography
Baud, D., Goy, G., Jaton, K., Osterheld, M.-C., Blumer, S., Borel, N., Vial, Y., Hohlfeld, P., Pospischil, A., and Greub, G. (2011). Role of Chlamydia trachomatis in miscarriage. Emerging Infectious Diseases 17, 1630-1635.
Falk, L., Fredlund, H., and Jensen, J.S. (2005). Signs and symptoms of urethritis and cervicitis among women with or without Mycoplasma genitalium or Chlamydia trachomatis infection. Sexually Transmitted Infections 81, 73-78.
Givan, A.L., White, H.D., Stern, J.E., Colby, E., Gosselin, E.J., Guyre, P.M., and Wira, C.R. (1997). Flow cytometric analysis of leukocytes in the human female reproductive tract: comparison of fallopian tube, uterus, cervix, and vagina. American Journal of Reproductive Immunology AJRI Official Journal of the American Society for the Immunology of Reproduction and the International Coordination Committee for Immunology of Reproduction 38, 350-359.
Hafner, L., Beagley, K., and Timms, P. (2008). Chlamydia trachomatis infection: host immune responses and potential vaccines. Mucosal Immunology 1, 116-130.
Hillis, S.D., Owens, L.M., Marchbanks, P. a, Amsterdam, L.F., and Mac Kenzie, W.R. (1997). Recurrent chlamydial infections increase the risks of hospitalization for ectopic pregnancy and pelvic inflammatory disease. American Journal of Obstetrics and Gynecology 176, 103-107.
Hosseinzadeh, S. (2003). Chlamydia trachomatis-induced death of human spermatozoa is caused primarily by lipopolysaccharide. Journal of Medical Microbiology 52, 193-200.
Howie, S.E.M., Horner, P.J., and Horne, A.W. (2011a). Chlamydia trachomatis infection during pregnancy: known unknowns. Discovery Medicine 12, 57-64.
Howie, S.E.M., Horner, P.J., Horne, A.W., and Entrican, G. (2011b). Immunity and vaccines against sexually transmitted Chlamydia trachomatis infection. Current Opinion in Infectious Diseases 24, 56-61.
Loomis, W.P., and Starnbach, M.N. (2002). T cell responses to Chlamydia trachomatis. Current Opinion in Microbiology 5, 87-91.
Manavi, K. (2006). A review on infection with Chlamydia trachomatis. Best Practice & Research. Clinical Obstetrics & Gynaecology 20, 941-951.
Paavonen, J., and Lehtinen, M. (1996). Chlamydial pelvic inflammatory disease. Human Reproduction Update 2, 519-529.
Perry, L.L., Feilzer, K., and Caldwell, H.D. (1997). Immunity to Chlamydia trachomatis is mediated by T helper 1 cells through IFN-gamma-dependent and -independent pathways. The Journal of Immunology 158, 3344-3352.
Shaw, J.L. V, Wills, G.S., Lee, K., Horner, P.J., Mcclure, M.O., Abrahams, V.M., Wheelhouse, N., Jabbour, H.N., Critchley, H.O.D., Entrican, G., et al. (2011). Chlamydia trachomatis Infection Increases Fallopian Tube PROKR2 via TLR2 and NF B Activation Resulting in a Microenvironment Predisposed to Ectopic Pregnancy. AJPA 178, 253-260.
Skerk, V. (2003). Comparative analysis of azithromycin and ciprofloxacin in the treatment of chronic prostatitis caused by Chlamydia trachomatis. International Journal of Antimicrobial Agents 21, 457-462.
Stamm, W.E., and Cole, B. (1986). Asymptomatic Chlamydia trachomatis urethritis in men. Sexually Transmitted Diseases 13, 163-165.
Wilkowska-Trojniel, M., Zdrodowska-Stefanow, B., Ostaszewska-Puchalska, I., Zbucka, M., Wolczynski, S., Grygoruk, C., Kuczynski, W., and Zdrodowski, M. (2009). Chlamydia trachomatis urogenital infection in women with infertility. Advances in Medical Sciences 54, 82-85.
© The copyright for this work resides with the author.